







Prematurity is the leading cause of death among children under five. Each year, approximately 15 million babies are born preterm, and more than 20 million are born low birthweight. These newborns face the highest risk of complications, yet a proven, accessible intervention dramatically improves their survival and development: Kangaroo Mother Care (KMC).
What the New WHO Clinical Practice Guide Confirms
The new WHO Kangaroo Mother Care: A Clinical Practice Guide provides updated global standards for clinical practice, facility readiness, and program implementation. It builds on the 2022 WHO recommendations and reinforces a clear message:
KMC is the essential standard of care for all preterm and low-birth-weight newborns.
It should begin as soon as possible after birth, even for newborns who need special or intensive care, unless they are in shock or unable to breathe on their own.
What KMC Includes
KMC is defined as:
-
Prolonged skin-to-skin contact (ideally 24 hours a day; minimum of 8 hours)
-
Exclusive breastfeeding or provision of breast milk
-
Care in an environment that enables mother and newborn to remain together continuously
This definition distinguishes KMC from routine early skin-to-skin contact immediately after birth.
Why Immediate KMC Matters
The updated guidance emphasizes immediate KMC—starting directly after birth. This shift is based on strong evidence showing that immediate KMC:
-
Reduces neonatal mortality
-
Reduces hypothermia
-
Lowers the risk of severe infections
-
Improves temperature regulation, breathing, and oxygenation
-
Increases breastfeeding initiation and duration
-
Improves long-term neurodevelopmental outcomes
-
Strengthens bonding and reduces stress for both parents and babies
-
Lowers healthcare costs and improves health system efficiency
Immediate and prolonged KMC creates the safest, most stable environment for infants who are born early or small.
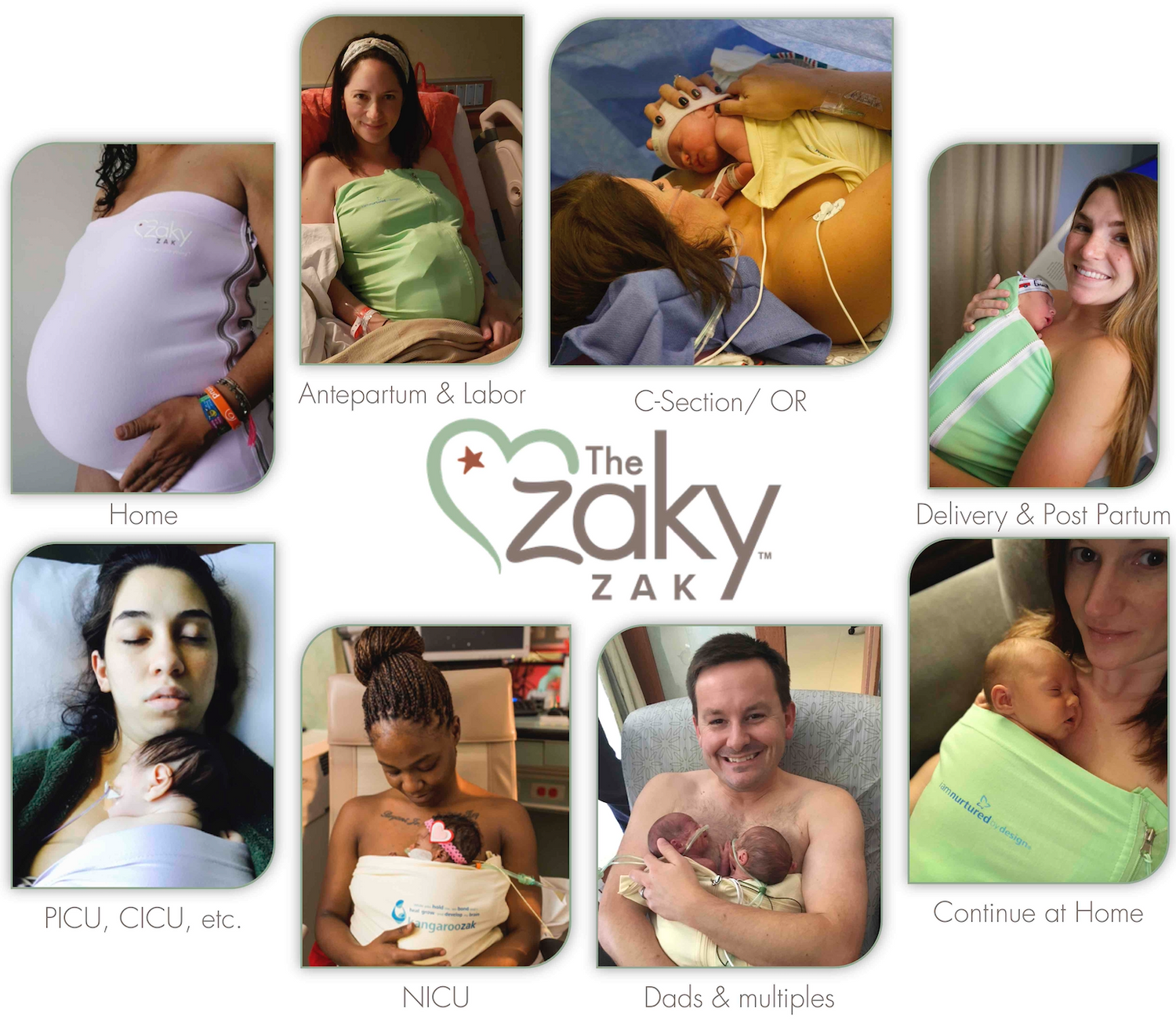
Who Provides KMC?
The mother is the primary caregiver for KMC, but fathers, grandparents, or another consistent caregiver may also participate. Additional caregivers ensure continuity of skin-to-skin contact when the mother needs rest or is recovering. This approach prevents unnecessary separation and supports family-integrated, trauma-informed care.
Where KMC Should Be Practiced
KMC can and should take place:
-
Immediately after birth in childbirth areas
-
In all levels of health facilities, including those providing special or intensive care
-
In mother–newborn care units, where mothers stay with newborns 24/7 while the baby receives clinical care
-
In dedicated KMC wards for clinically improving infants
-
At home after discharge, or starting at home for eligible babies who do not require facility-based intensive care
The guide outlines what facilities need to implement KMC safely and consistently, including appropriate infrastructure, staff training, monitoring, and policies.
How Long Should KMC Continue
KMC continues for as long as the newborn accepts it. In most cases, babies maintain KMC comfortably until around 38–40 weeks corrected gestational age or approximately 2,500 grams. Babies naturally begin to “wriggle out” of the position when they are mature enough to regulate their own temperature and maintain stable physiology without continuous skin-to-skin support.
A Global, Multi-Stakeholder Effort
The updated WHO guidance was developed through collaboration with government program leaders, clinicians, scientists, parent organizations, NGOs, professional associations, donors, and global partnerships. It represents a unified commitment to ensuring that every preterm or low-birth-weight newborn receives the life-saving benefits of KMC from birth.
Looking Ahead: A Commitment to Zero Separation
Kangaroo Mother Care is not an optional add-on. It is a life-saving, development-shaping, and cost-effective standard of care that centers love, safety, stability, and connection.
At kangaroo.care, we are committed to sharing this global guidance and promoting practices that keep parents and newborns together—because healing begins when they are held close.
 |
|
 |
|
 |
|
|
 |